Risks, side effects and why modern anaesthesia is much safer than it used to be
A useful way to think about risk is to separate common temporary side effects from genuinely serious complications. The two are not the same.
Common and usually temporary
- Drowsiness or grogginess
- Sore throat or hoarse voice
- Nausea or vomiting
- Shivering, dizziness or blurred thinking
- Ache or bruise at the cannula site
- Mild confusion or vivid dreams for a short time
Rare but important
- Severe allergic reaction (anaphylaxis)
- Breathing problems or aspiration
- Dental injury or airway trauma
- Awareness under anaesthesia in selected higher-risk settings
- Major heart, brain or lung complications, often tied more to the patient and surgery than to the anaesthetic alone
- Malignant hyperthermia in susceptible patients exposed to triggering agents
Why outcomes are better than 50 years ago
Major improvements have come from routine pulse oximetry, capnography, better airway devices, safer machines, standard monitoring, video laryngoscopes, ultrasound for vascular access and nerve blocks, better drugs, formal recovery care, and stronger training and safety systems. In selected cases, processed EEG or BIS-style monitoring may also be used to help judge hypnotic depth.
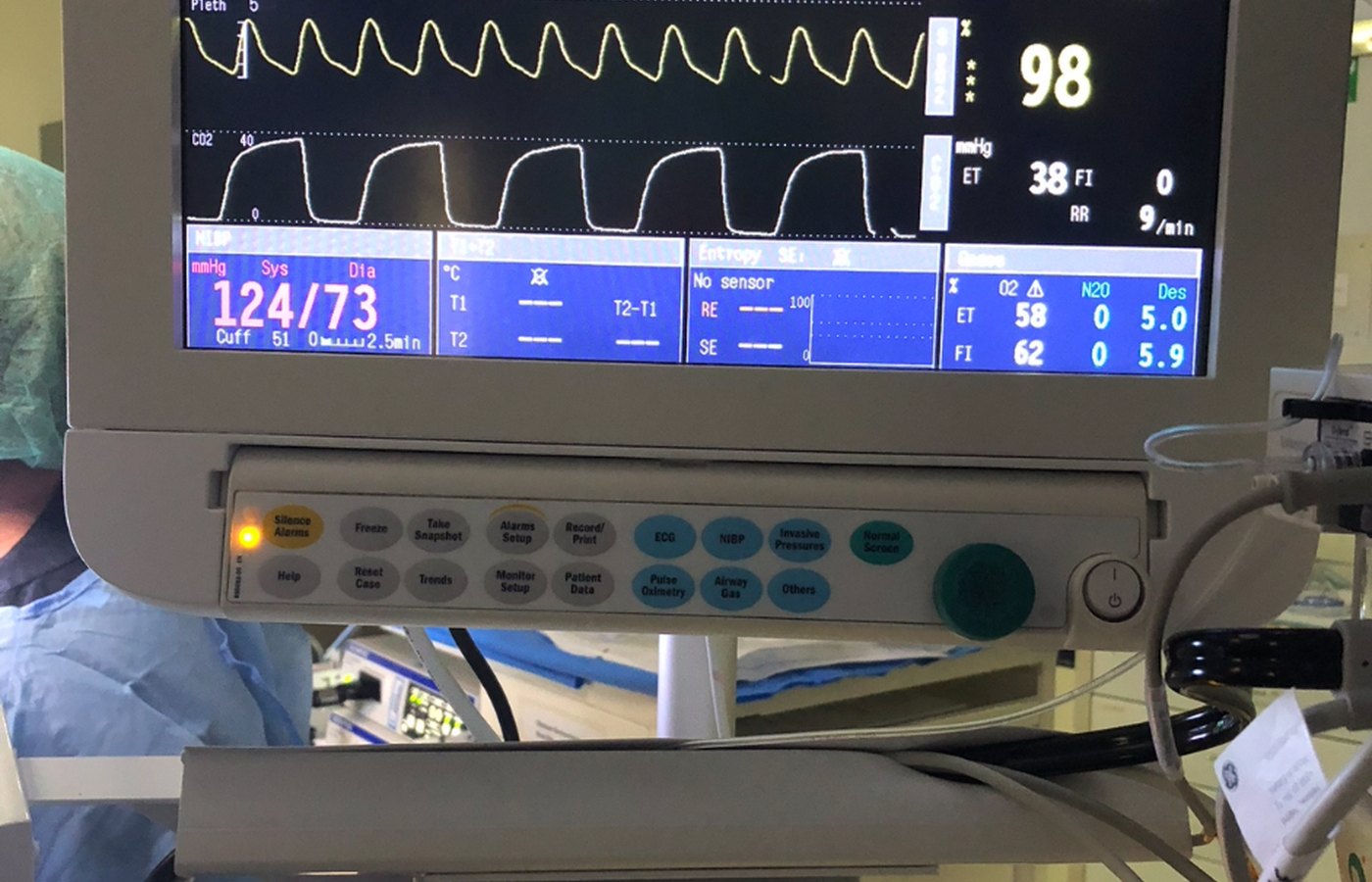
Pulse oximetry
Continuous oxygen saturation monitoring helps detect hypoxaemia early.
Capnography
Continuous carbon dioxide monitoring helps show whether you are breathing effectively and whether the airway circuit is working as intended.
Airway and regional advances
Video laryngoscopy and ultrasound have improved many aspects of airway care, vascular access and regional anaesthesia.
Putting risk in perspective
Routine anaesthesia for healthy people is generally safer than many people imagine from anecdotes. Everyday life already contains risk in transport, sport and other activities. That does not make medical risk irrelevant, but it does mean you should not let sensational stories dominate your judgment. Your own risk depends on the operation, urgency, age, weight, airway, pregnancy status, reflux, sleep apnoea, medications and underlying disease.
Malignant hyperthermia
This is an uncommon inherited reaction to specific triggering anaesthetic agents. If there is a personal or family history, tell the anaesthetist. Susceptible patients can still have surgery safely, but the anaesthetic plan changes and triggering agents are avoided.
Pseudocholinesterase deficiency
This can lead to unexpectedly prolonged paralysis after certain muscle relaxants such as succinylcholine and mivacurium. It is rare, but a family history can be highly relevant.